
MRI of the Brain and Cerebellopontine Angle (CPA MRI)
MRI of the brain and cerebellopontine angle (CPA MRI) is a specialized neuroimaging examination used to evaluate the posterior cranial fossa, cerebellopontine angle cisterns, internal auditory canals, brainstem, cerebellum, cranial nerves, and adjacent vascular structures. This examination is especially important when symptoms suggest pathology of the vestibulocochlear nerve, facial nerve, trigeminal nerve, internal auditory canal, or posterior fossa structures.
CPA MRI is not only a “tumor search” examination. It is a detailed neuroradiological assessment of small anatomical structures where very small lesions may cause significant symptoms such as unilateral hearing loss, tinnitus, vertigo, imbalance, facial numbness, trigeminal neuralgia, facial weakness, or hemifacial spasm.
MRI of the cerebellopontine angle should be understood as an advanced extension of a complete brain MRI examination. Standard neuro MRI evaluates the brain as a whole, while dedicated CPA and internal auditory canal imaging focuses on cranial nerves, small tumors, neurovascular conflict, and pathology of the posterior fossa.
What Is the Cerebellopontine Angle?
The cerebellopontine angle is an anatomical space located in the posterior cranial fossa between the pons, cerebellum, and petrous temporal bone. It contains cerebrospinal fluid, cranial nerves, vascular structures, and the entrance to the internal auditory canal. Because many important nerves pass through this region, even a small lesion can cause clinically significant symptoms.
The CPA region is closely related to hearing, balance, facial movement, facial sensation, eye movement coordination, and brainstem function. Dedicated high-resolution MRI is the preferred imaging method for evaluating this complex region because it provides excellent soft-tissue contrast and allows detailed visualization of nerves, vessels, tumors, cysts, and inflammatory changes.
Anatomy of the Cerebellopontine Angle on MRI
High-resolution MRI of the cerebellopontine angle evaluates both the CPA cistern and the adjacent posterior fossa structures. Important anatomical landmarks include:
- pons and pontomedullary junction;
- middle cerebellar peduncle;
- cerebellar hemisphere and cerebellar flocculus;
- internal auditory canal;
- cerebellopontine angle cistern;
- subarachnoid cerebrospinal fluid spaces;
- facial nerve;
- vestibulocochlear nerve;
- trigeminal nerve;
- lower cranial nerves in adjacent skull base regions;
- anterior inferior cerebellar artery;
- posterior inferior cerebellar artery;
- superior cerebellar artery;
- vertebrobasilar arterial system;
- petrous temporal bone and labyrinthine structures.
Which Structures Are Evaluated During CPA MRI?
A dedicated MRI examination of the cerebellopontine angle and internal auditory canal evaluates the relationship between nerves, vessels, cerebrospinal fluid spaces, brainstem, cerebellum, and skull base structures.
- cerebellopontine angle cisterns;
- internal auditory canals;
- facial nerve pathways;
- vestibulocochlear nerves;
- cochlear and vestibular nerve divisions when visible;
- trigeminal nerve root entry zone;
- brainstem and pons;
- cerebellum and middle cerebellar peduncles;
- labyrinthine region and inner ear structures when included in the field of view;
- vascular loops and neurovascular relationships;
- posterior fossa meninges;
- extra-axial masses, cysts, inflammatory lesions, and vascular abnormalities.
Which Cranial Nerves Pass Through the CPA Region?
The cerebellopontine angle is anatomically important because several cranial nerves are located in or near this region. The most clinically relevant nerves for CPA MRI are:
- cranial nerve V — trigeminal nerve;
- cranial nerve VII — facial nerve;
- cranial nerve VIII — vestibulocochlear nerve;
- lower cranial nerves IX, X, and XI in adjacent jugular foramen and lower posterior fossa regions.
The trigeminal nerve is assessed in patients with facial pain, trigeminal neuralgia, sensory disturbance, or suspected neurovascular conflict. The facial nerve is assessed in facial weakness, hemifacial spasm, facial nerve tumors, and inflammatory neuropathy. The vestibulocochlear nerve is evaluated in unilateral hearing loss, tinnitus, vestibular schwannoma, dizziness, and balance disorders.
VII and VIII Cranial Nerves on CPA MRI
The facial nerve (cranial nerve VII) and vestibulocochlear nerve (cranial nerve VIII) travel together from the brainstem through the cerebellopontine angle cistern into the internal auditory canal. Their close anatomical relationship explains why CPA and internal auditory canal lesions may produce combined symptoms involving facial movement, hearing, and balance.
Facial Nerve (Cranial Nerve VII)
The facial nerve controls muscles of facial expression and carries parasympathetic and sensory fibers. MRI may evaluate the facial nerve in cases of facial weakness, facial nerve enhancement, inflammatory neuritis, facial nerve schwannoma, hemifacial spasm, postoperative changes, and neurovascular compression near the root exit zone.
Vestibulocochlear Nerve (Cranial Nerve VIII)
The vestibulocochlear nerve consists of cochlear and vestibular components. It is responsible for hearing and balance. MRI of the internal auditory canal is essential for detecting vestibular schwannoma, cochlear schwannoma, labyrinthine schwannoma, inflammatory nerve enhancement, and other lesions affecting hearing or vestibular function.
How CPA MRI Differs From Standard Brain MRI
Standard brain MRI evaluates the whole brain, including the cerebral cortex, white matter, basal ganglia, brainstem, cerebellum, ventricular system, cerebrospinal fluid spaces, meninges, and major intracranial structures. However, routine brain MRI may not provide sufficient spatial resolution for small cranial nerves, internal auditory canal lesions, tiny vestibular schwannomas, or subtle neurovascular conflict.
CPA MRI differs from routine brain MRI because it uses:
- thin-slice high-resolution imaging;
- small field-of-view sequences;
- dedicated internal auditory canal imaging;
- 3D heavily T2-weighted sequences such as CISS, FIESTA, or DRIVE;
- targeted post-contrast assessment;
- multiplanar reconstructions;
- focused evaluation of cranial nerves and vascular loops.
Why CPA MRI Should Be Performed Together With Complete Brain MRI
CPA MRI does not replace a complete brain MRI examination. A full neuro MRI examination evaluates the cerebral cortex, white matter, brainstem, cerebellum, ventricular system, cerebrospinal fluid spaces, vessels, and meninges. After this general assessment, dedicated CPA and cranial nerve imaging can be performed to evaluate the internal auditory canals, CPA cisterns, and small neurovascular structures.
An isolated CPA examination may be insufficient because symptoms such as dizziness, tinnitus, hearing loss, facial numbness, facial weakness, imbalance, or headache may be caused by pathology outside the cerebellopontine angle. Possible alternative locations include the brainstem, cerebellum, temporal lobes, demyelinating plaques, vascular lesions, inflammatory disease, or intracranial masses outside the CPA.
Comprehensive brain MRI increases diagnostic accuracy because it allows correlation between focal CPA findings and the broader intracranial context.
Which MRI Sequences Are Used in CPA MRI?
T1-Weighted Imaging
T1-weighted imaging provides anatomical detail and helps evaluate fat, hemorrhage, solid tumor components, postoperative changes, and pre-contrast baseline signal. It is also essential for comparison with post-contrast T1-weighted images.
T2-Weighted Imaging
T2-weighted imaging demonstrates cerebrospinal fluid spaces, cystic lesions, edema, tumor morphology, brainstem abnormalities, and inner ear fluid-containing structures.
FLAIR Imaging
FLAIR suppresses cerebrospinal fluid signal and helps detect inflammatory, demyelinating, ischemic, gliotic, or leptomeningeal abnormalities that may affect the brainstem, cerebellum, or adjacent brain tissue.
DWI and ADC
Diffusion-weighted imaging and ADC maps are important for differentiating epidermoid cysts from arachnoid cysts, identifying acute ischemia, detecting abscesses, and assessing cellular lesions.
SWI
Susceptibility-weighted imaging helps detect microhemorrhage, cavernomas, hemosiderin, calcification, venous abnormalities, and hemorrhagic components of lesions.
T1 Post-Contrast Imaging
Contrast-enhanced T1-weighted imaging is essential for detecting vestibular schwannoma, meningioma, inflammatory enhancement, metastases, facial or vestibulocochlear nerve enhancement, leptomeningeal disease, and postoperative recurrence.
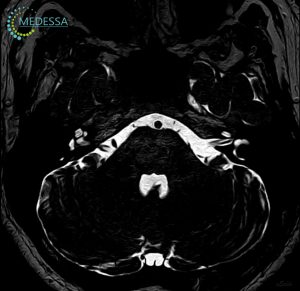
3D CISS / FIESTA / DRIVE
3D CISS, FIESTA, and DRIVE are high-resolution heavily T2-weighted steady-state sequences that provide excellent contrast between cerebrospinal fluid and small cranial nerves. They are particularly valuable for evaluating the internal auditory canal, facial nerve, vestibulocochlear nerve, trigeminal nerve, small CPA lesions, and neurovascular contact.
3D CISS, FIESTA, and DRIVE Sequences in CPA MRI
3D CISS, FIESTA, and DRIVE sequences are among the most important technical components of high-quality CPA MRI. These sequences allow thin-slice volumetric imaging with multiplanar reconstruction and high contrast between nerves, vessels, and cerebrospinal fluid.
They are used to evaluate:
- facial nerve and vestibulocochlear nerve in the internal auditory canal;
- trigeminal nerve root entry zone;
- vascular loops contacting cranial nerves;
- small vestibular schwannomas;
- neurovascular conflict;
- tiny intracanalicular lesions;
- posterior fossa cysts and extra-axial lesions;
- relationship between nerves, vessels, and CSF spaces.
Thin slices reduce partial volume artifacts and improve detection of subtle abnormalities. High spatial resolution is essential because cranial nerves and small intracanalicular lesions may measure only a few millimeters.
MRI of the Internal Auditory Canal
MRI of the internal auditory canal is a targeted assessment of the bony canal that contains the facial nerve, cochlear nerve, superior vestibular nerve, inferior vestibular nerve, and labyrinthine vessels. It is commonly performed in patients with unilateral sensorineural hearing loss, tinnitus, vertigo, dizziness, imbalance, facial nerve symptoms, or suspected vestibular schwannoma.
Internal auditory canal MRI evaluates:
- intracanalicular vestibular schwannoma;
- cochlear nerve abnormalities;
- facial nerve enhancement;
- labyrinthine schwannoma;
- inflammatory neuritis;
- meningeal enhancement;
- small enhancing lesions;
- asymmetry of internal auditory canal contents.
What Diseases Can Be Detected With CPA MRI?
Vestibular Schwannoma
Vestibular schwannoma is a benign nerve sheath tumor arising from the vestibular component of the vestibulocochlear nerve. MRI evaluates its size, intracanalicular extension, CPA component, brainstem compression, contrast enhancement, and relationship to the internal auditory canal.
Acoustic Neuroma
Acoustic neuroma is a commonly used historical term for vestibular schwannoma. Although the tumor usually arises from the vestibular nerve rather than the cochlear nerve, the term remains widely used in patient searches.
Meningioma
CPA meningiomas are extra-axial tumors that may mimic vestibular schwannoma but often have a broad dural attachment, dural tail, and different relationship to the internal auditory canal.
Epidermoid Cyst
Epidermoid cysts may occur in the CPA and typically show diffusion restriction on DWI, helping differentiate them from arachnoid cysts.
Arachnoid Cyst
Arachnoid cysts follow cerebrospinal fluid signal and usually do not restrict diffusion. MRI helps define mass effect and relationship to cranial nerves.
Neurovascular Conflict
Neurovascular conflict occurs when a vessel contacts or compresses a cranial nerve, most often at the nerve root entry or exit zone. MRI helps evaluate the relationship between arteries and nerves.
Trigeminal Neuralgia
MRI evaluates the trigeminal nerve, root entry zone, vascular compression, tumors, demyelinating plaques, and other secondary causes of trigeminal neuralgia.
Facial Nerve Compression and Hemifacial Spasm
Hemifacial spasm may be associated with vascular compression of the facial nerve near its root exit zone. High-resolution MRI can identify vascular contact and support surgical planning.
Demyelinating Disease
Demyelinating plaques in the brainstem or trigeminal pathways may cause facial sensory symptoms, vertigo, diplopia, or neuralgia-like pain.
Inflammatory and Infectious Changes
MRI can detect neuritis, leptomeningeal enhancement, inflammatory enhancement of cranial nerves, labyrinthitis, and skull base inflammatory processes.
Metastatic Lesions
Metastases may involve the CPA, internal auditory canal, meninges, cranial nerves, or skull base. Contrast-enhanced MRI is especially important when metastatic disease is suspected.
MRI for Acoustic Neuroma and Vestibular Schwannoma
MRI is the preferred imaging method for vestibular schwannoma because it can detect small intracanalicular tumors, define extension into the CPA cistern, evaluate tumor size, assess contrast enhancement, and demonstrate relationship to the brainstem, cerebellum, internal auditory canal, facial nerve, and vestibulocochlear nerve.
Important MRI features include:
- intracanalicular component;
- CPA extension;
- tumor size and volume;
- contrast enhancement pattern;
- cystic degeneration;
- brainstem or cerebellar compression;
- hydrocephalus in large tumors;
- relationship to the facial nerve and cochlear nerve;
- bilateral lesions in suspected neurofibromatosis type 2.
MRI findings are important for choosing observation, radiosurgery, microsurgery, or follow-up strategy. Serial MRI is used to monitor tumor growth and treatment response.
MRI for Neurovascular Conflict
MRI for neurovascular conflict is used to evaluate contact or compression between vessels and cranial nerves. The most common clinical scenarios include trigeminal neuralgia, hemifacial spasm, and vestibular paroxysmia.
High-resolution 3D CISS, FIESTA, or DRIVE sequences are especially valuable because they show the cisternal segments of cranial nerves surrounded by cerebrospinal fluid and demonstrate nearby vascular loops.
MRI may evaluate:
- compression of the trigeminal nerve by the superior cerebellar artery or other vessels;
- compression of the facial nerve by vascular loops near the root exit zone;
- contact between artery and nerve;
- nerve displacement, distortion, or atrophy;
- vascular loops in the internal auditory canal region;
- anatomy relevant to microvascular decompression planning.
Neurovascular contact alone does not always prove symptoms are caused by compression. MRI findings must be correlated with clinical presentation and neurological evaluation.
MRI for Trigeminal Neuralgia
Trigeminal neuralgia is characterized by recurrent brief attacks of severe facial pain in the distribution of one or more branches of the trigeminal nerve. MRI is used to evaluate neurovascular compression and exclude secondary causes such as tumors, multiple sclerosis plaques, aneurysms, epidermoid cysts, meningiomas, or inflammatory lesions.
Dedicated trigeminal nerve imaging assesses the cisternal segment, root entry zone, Meckel’s cave, cavernous sinus, skull base foramina, and brainstem pathways.
MRI for Hemifacial Spasm
Hemifacial spasm may occur when a vascular loop compresses the facial nerve near the brainstem. MRI helps visualize the facial nerve root exit zone and its relationship to adjacent vessels. This information may be relevant for treatment planning, including microvascular decompression in selected cases.
MRI for Tinnitus
MRI may be recommended in unilateral tinnitus, asymmetric hearing loss, pulsatile tinnitus, or tinnitus associated with neurological symptoms. MRI can detect vestibular schwannoma, internal auditory canal lesions, vascular abnormalities, inflammatory disease, demyelinating lesions, or posterior fossa pathology.
MRI for Unilateral Hearing Loss
Unilateral sensorineural hearing loss is one of the most common indications for internal auditory canal MRI. The purpose is to exclude vestibular schwannoma and other retrocochlear pathology affecting the cochlear nerve, vestibular nerve, internal auditory canal, CPA cistern, or brainstem auditory pathways.
MRI for Dizziness, Vertigo, and Balance Disorders
Dizziness and balance disorders may arise from inner ear, vestibular nerve, brainstem, cerebellar, vascular, inflammatory, or central nervous system causes. CPA MRI helps evaluate vestibular schwannoma, brainstem lesions, cerebellar pathology, demyelination, posterior circulation abnormalities, and cranial nerve disorders.
Why 3.0 Tesla and 1.5 Tesla Matter in CPA MRI
MRI of the cerebellopontine angle, internal auditory canal, and cranial nerves is technically demanding because the structures are very small and located near dense skull base anatomy. Both 1.5 Tesla and 3.0 Tesla MRI systems can be used for CPA imaging when protocols are optimized.
Advantages of 3.0 Tesla MRI
- higher signal-to-noise ratio;
- better cranial nerve visualization;
- improved detection of very small lesions;
- better visualization of neurovascular conflict;
- higher spatial resolution in the internal auditory canal;
- improved posterior fossa imaging;
- more detailed assessment of the facial nerve and vestibulocochlear nerve;
- better performance of thin-slice 3D CISS, FIESTA, and DRIVE sequences.
Role of 1.5 Tesla MRI
Modern 1.5 Tesla MRI can also provide clinically valuable CPA imaging, especially when dedicated high-resolution protocols are used. Many vestibular schwannomas, meningiomas, cysts, inflammatory lesions, and internal auditory canal abnormalities can be reliably evaluated at 1.5 Tesla.
Diagnostic quality depends not only on magnetic field strength, but also on protocol optimization, thin-slice acquisition, motion control, contrast use when indicated, radiologist expertise, and clinical information.
Related MRI Examinations
Frequently Asked Questions (FAQ)
What does CPA MRI show?
CPA MRI shows the cerebellopontine angle cisterns, internal auditory canals, facial nerve, vestibulocochlear nerve, trigeminal nerve, brainstem, cerebellum, posterior fossa vessels, and surrounding skull base structures. It can detect vestibular schwannoma, meningioma, epidermoid cyst, arachnoid cyst, neurovascular conflict, inflammation, metastases, and internal auditory canal pathology.
What is the cerebellopontine angle?
The cerebellopontine angle is a cerebrospinal fluid-filled anatomical space in the posterior cranial fossa between the pons, cerebellum, and petrous temporal bone. It contains important cranial nerves and vessels related to hearing, balance, facial movement, and facial sensation.
Can MRI detect acoustic neuroma?
Yes. MRI is the preferred imaging method for detecting acoustic neuroma, also known as vestibular schwannoma. It can identify small intracanalicular tumors and larger lesions extending into the cerebellopontine angle.
Can MRI show the trigeminal nerve?
Yes. High-resolution MRI sequences such as CISS, FIESTA, or DRIVE can visualize the cisternal segment of the trigeminal nerve and assess neurovascular contact, tumors, demyelination, or other causes of trigeminal neuralgia.
What is neurovascular conflict?
Neurovascular conflict is contact or compression between a blood vessel and a cranial nerve. It may be associated with trigeminal neuralgia, hemifacial spasm, or vestibular symptoms, but MRI findings must always be interpreted together with clinical symptoms.
Is contrast needed for CPA MRI?
Contrast is often important when evaluating vestibular schwannoma, meningioma, inflammatory nerve enhancement, metastases, postoperative changes, or unclear CPA lesions. Non-contrast high-resolution sequences are also essential for nerve and vessel anatomy.
What is vestibular schwannoma?
Vestibular schwannoma is a benign nerve sheath tumor that usually arises from the vestibular component of the vestibulocochlear nerve. It may cause unilateral hearing loss, tinnitus, dizziness, imbalance, or compression of nearby structures.
Can a small CPA tumor be missed?
Small intracanalicular tumors may be difficult to detect without dedicated internal auditory canal imaging, thin slices, contrast-enhanced sequences, and high-resolution 3D CISS, FIESTA, or DRIVE imaging.
Why is 3.0 Tesla MRI useful for CPA imaging?
3.0 Tesla MRI provides higher signal-to-noise ratio, better cranial nerve visualization, improved internal auditory canal imaging, and better detection of very small lesions or neurovascular conflict.
Can CPA MRI be performed at 1.5 Tesla?
Yes. A well-optimized 1.5 Tesla MRI protocol can provide clinically valuable information for many CPA and internal auditory canal diseases. Protocol quality and radiologist expertise are very important.
What are CISS, FIESTA, and DRIVE sequences?
CISS, FIESTA, and DRIVE are high-resolution heavily T2-weighted 3D MRI sequences that show cranial nerves and vessels against bright cerebrospinal fluid. They are essential for internal auditory canal and neurovascular conflict imaging.
Why does tinnitus require MRI?
MRI may be recommended for unilateral tinnitus, asymmetric hearing loss, pulsatile tinnitus, or tinnitus with neurological symptoms to exclude vestibular schwannoma, vascular abnormalities, demyelination, inflammatory disease, or posterior fossa pathology.
Why can dizziness or vertigo require CPA MRI?
Dizziness and vertigo may be caused by vestibular nerve lesions, vestibular schwannoma, brainstem pathology, cerebellar disease, demyelination, inflammation, or vascular abnormalities. CPA MRI helps evaluate central and retrocochlear causes.
Can children undergo CPA MRI?
Yes. CPA MRI can be performed in children when clinically indicated. Young children may require special preparation or sedation if they cannot remain still during scanning.
How long does CPA MRI take?
The duration depends on the protocol, need for contrast, use of high-resolution 3D sequences, and whether full brain MRI and vascular imaging are included.
How is CPA MRI different from routine brain MRI?
CPA MRI includes dedicated thin-slice internal auditory canal imaging, high-resolution cranial nerve sequences, and targeted assessment of the cerebellopontine angle. Routine brain MRI may not be detailed enough for small CPA lesions or neurovascular conflict.
Can MRI detect hemifacial spasm causes?
Yes. MRI can evaluate the facial nerve root exit zone and identify vascular contact or compression that may be associated with hemifacial spasm.
Can MRI detect the cause of unilateral hearing loss?
Yes. MRI of the internal auditory canals is commonly used to exclude vestibular schwannoma and other retrocochlear causes of unilateral sensorineural hearing loss.
Does CPA MRI replace a full brain MRI?
No. CPA MRI is a targeted extension of brain MRI. A complete brain MRI is important because symptoms may originate from the brainstem, cerebellum, demyelinating disease, vascular lesions, or other intracranial pathology outside the CPA.